FLEXIBLE IOLS
SILICONE
-
Introduced in 1984 as a foldable IOL material
-
Used in order to make corneal incision size smaller during IOL implantation
-
Polymers consist of silicone and oxygen
-
High refractive index, therefore allowing thinner IOL optics
-
-
Hydrophobic
-
Wettability angle of 99º
-
N.B. Wettability angle is the contact angle
-
between a solid and liquid
-
IOL implantation can be difficult due to the slippery nature of silicone's surface when wet
-
Therefore handled dry during surgery
-
-
Currently, 3-piece models are used
-
With haptics made of PMMA, PVDF or Polyamide
-
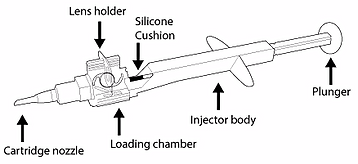
Injectors have been developed for insertion of these lenses
-
Allowing for easier handling
-
-
When silicone IOLs are inserted into the capsular bag, they tend to unfold rapidly and uncontrollably
-
This increases the likelihood of intraocular damage
-
-
Bacteria adhesion in these lenses has also been known
-
This has lead to an increased risk of post-surgery infection
-
-
Once implanted, anterior capsular opacification (ACO) and inflammation occurs
-
Rate of ACO is higher in IOLs with a plate-haptic design
-
This is due to the large contact area between the silicone material
-
and anterior capsule
-
This stimulates cell proliferation and fibrosis
-
The posterior capsule remains clear for several years
-
This is due to the low adhesion to extracellular components which cause this form of opacification (PCO)
-
-
Less commonly used material
-
Not suitable for Microincision Cataract Surgery (MICS)
-
This is due to the larger corneal incision silicone IOLs require
-
-
More recently, a silicone IOL was created, in which UV exposure is used to change the power post-implantation.
-
Silicone oil is used as a tamponading agent
-
This agent, without leaking through retinal tears,
-
acts as a 'plug' in retinal detachment surgery
-
However, silicone droplets are known to stick to the
the posterior IOL surface
-
YAG capsulotomy is used to remove the oil, causing
silicone droplets to deposit onto the posterior IOL
surface
-
This means the IOL needs to be replaced
ACRYLIC
HYDROPHOBIC FOLDABLE ACRYLIC
-
Have the ability to be folded, pushed and pulled
-
No permanent structure changes occur
-
-
Copolymers of acrylate and methacrylate are derived from PMMA
-
Therefore make the material flexible and durable
-
-
Lens optic diameter: 5.5 -7.0mm
-
Overall length: 12 - 13mm
-
High refractive index
-
Therefore, thin and foldable
-
Able to pass through a small incision (2.2mm)
-
-
Associated with photopsia because of the high index
-
and low anterior curvatures
-
Wettability angle: smaller than silicone, measuring at 73º
-
Low water content
-
Soft copolymers
-
Prone to scratches and permanent fingerprints
-
Known to decentre, therefore surgeons must be extra cautious during implantation
-
-
There has been less PCO found, and withstanding considerable damage from YAG capsulotomy
-
Acrylic IOLs do not attract silicone droplet deposits from silicone oil
-
-
'Glistenings' have been reported
-
Newer materials have been introduced to prevent further uptake of water
-
HYDROPHILIC FOLDABLE ACRYLIC
-
Most common material for IOLs
-
Consists of a mixture of hydroxyethylmethacrylate (poly-HEMA) and hydrophilic acrylic monomer
-
Refractive index: 1.43
-
Most lenses have a water content ranging between 18 and 26%
-
Wettability angle of 50º
-
Because of their hydrophilic surface, the IOLs are soft and
-
have good biocompatibility
-
The flexible surface means that there is minimal damage to the folding and insertion of lens
-
For implantation of the IOL, the corneal incision required only needs to measure 2mm or less
-
Therefore, an appropriate choice for MICS
-
-
These lenses are advantageous to surgeons as they are easier to handle
-
Also have been known to rarely dislocate if implanted accurately
-
-
Following surgery, PCO occurs at a higher rate that other materials such as silicone and hydrophobic acrylics
-
If YAG capsulotomy is carried out, the lens is more susceptible for laser damage
-
-
The incidence of photopsia is low in comparison to lenses of a hydrophobic nature
-
But there is a concern of optic opacification due to calcium deposits
-
This concern has been associated with, but may not be due to, certain IOL types
-
-
COLLAMER
-
Combination of 'collagen' and 'polymer'
-
Produced by STAAR surgical
-
Water content: 40%
-
Collamer is soft and IOLs are able to unfold slowly
-
Therefore, implantation is easier
-
-
-
Collamer combines the best components of silicone and acrylic lenses
-
Higher refractive index than silicone (1.442), so can be folded into an even smaller arrangement
-
The procedure can be carried out through a smaller corneal incision
-
-
It is a negatively charged and hydrophilic material, thus is required to stay wet during surgery
-
Due to the low elastic memory of Collamer, it is 'pushed out' of the injection cartridge, giving more control to the surgeon
-
-
Post-surgical inflammation of the eye is absent with this material
-
Collamer attracts a protein known as fibronectin, forming a layer around the IOL, enabling the lens to be 'shielded' from attack from the body's immune system
-